A Cajun seafood boil is the kind of dinner that turns the table into the event: sweet shrimp, juicy crab legs, smoky sausage, corn, potatoes, lemon, garlic, Cajun seasoning, and a glossy garlic butter sauce that gets into every shell, every potato, and every bite of corn.
Timing is the part that makes people nervous. Seafood is expensive, shrimp overcooks fast, crab legs are often already cooked, and potatoes need a head start if you want them seasoned all the way through. This recipe keeps the feast feeling big, but the method stays calm: build a bold broth, add everything in the right order, save a little broth for the sauce, then finish the whole tray with Cajun garlic butter.
This recipe works as your main home-kitchen seafood boil: shrimp or prawns, crab legs, smoked sausage, corn, potatoes, Cajun seasoning, and garlic butter sauce. Crawfish, lobster tails, mussels, and clams can join the pot, but they are not required for a saucy, satisfying boil.
Quick Answer: How Do You Make a Cajun Seafood Boil?
A Cajun seafood boil is made by simmering potatoes, sausage, corn, crab legs, and shrimp in a seasoned Cajun broth, then finishing everything with garlic butter sauce. Cook the ingredients in stages: potatoes first, sausage next, corn and crab after that, and shrimp last. Reserve some broth for the butter sauce before draining.
A 6-serving home version uses a 10 to 12 quart / 9.5 to 11.4 L pot, about 4 quarts / 3.8 L total liquid, 2 lb / 900 g crab legs, 1.5 to 2 lb / 680 to 900 g shrimp, 12 to 14 oz / 340 to 400 g sausage, 1.5 lb / 680 g baby potatoes, and 4 to 6 ears of corn.
Simple rule: potatoes early, shrimp last, sauce at the end. That one order keeps the potatoes flavorful, the crab sweet, and the shrimp tender instead of rubbery.
Even if this is your first seafood boil, you do not have to manage everything at once. Prep first, cook in stages, and keep the shrimp for the very end. The pot builds flavor; the sauce delivers it.
Best first-time path: make the classic shrimp-and-crab version, use the normal coating sauce, keep the heat medium, and skip a long soak. This gives you a full, saucy tray without overcomplicating the pot.

Cajun Seafood Boil Recipe Card
Cajun Seafood Boil With Garlic Butter Sauce
A bold home-kitchen Cajun seafood boil with shrimp, crab legs, smoked sausage, corn, potatoes, lemon, garlic, Cajun seasoning, and buttery garlic sauce. The ingredients move in stages so the potatoes absorb the broth, the crab heats gently, and the shrimp stays tender.

| Prep Time | 20 minutes |
| Cook Time | 35 minutes |
| Total Time | 55 minutes, plus 5 to 10 minutes if soaking |
| Servings | 6 |
| Method | Stovetop |
| Pot Size | 10 to 12 quart / 9.5 to 11.4 L stockpot |
| Best Cue | Shrimp just cooked; potatoes tender; crab heated through |
Seafood Boil Ingredients
- 4 quarts / 3.8 L total liquid: water, or mostly water plus 12 oz / 355 ml beer
- 1 large onion, quartered
- 1 to 2 heads garlic, halved crosswise
- 2 lemons, halved, plus extra wedges for serving
- 2 to 3 bay leaves
- 1/4 cup Cajun seasoning to start, up to 1/2 cup only if your blend is low-salt or salt-free
- 1 to 2 tablespoons Old Bay or seafood seasoning, optional
- 1.5 lb / 680 g baby potatoes
- 12 to 14 oz / 340 to 400 g andouille or smoked sausage, sliced into thick rounds
- 4 to 6 ears corn, cut into halves or thirds
- 2 lb / 900 g snow crab legs or crab clusters, usually precooked
- 1.5 to 2 lb / 680 to 900 g jumbo raw shrimp or prawns, easy-peel or deveined shell-on if possible
- Salt, only if needed after tasting the broth
- Fresh parsley, for serving
Why the seasoning amount looks large: this seasons the water, potatoes, corn, shells, and seafood, not just the surface of the shrimp. Start with 1/4 cup if your blend contains salt.
Optional Add-Ins
- 1 to 2 lb / 450 to 900 g cooked or properly prepared crawfish; for live crawfish, use crawfish-specific cleaning and cooking guidance
- 2 to 3 lobster tails
- 1 lb / 450 g mussels or clams, cleaned
- 4 to 6 peeled hard-boiled eggs, warm or room-temperature, added after draining
Cajun Garlic Butter Sauce
- 1 cup / 227 g unsalted butter
- 6 to 8 garlic cloves, finely minced
- 1 tablespoon Cajun seasoning
- 1 teaspoon smoked paprika
- 1 to 2 tablespoons lemon juice
- 1/4 to 1/2 cup / 60 to 120 ml reserved seafood boil broth
- 1 to 2 teaspoons hot sauce, optional
- 2 tablespoons chopped parsley
Method
- Prep everything first. Cut the corn, slice the sausage, halve the lemons and garlic, rinse the seafood, and thaw frozen seafood if needed.
- Build the broth. Add the liquid, onion, garlic, lemons, bay leaves, 1/4 cup Cajun seasoning, and optional Old Bay to a large stockpot. Bring to a rolling boil and simmer for 5 to 10 minutes, until it smells garlicky, lemony, and spicy.
- Taste the broth. It should be bold, but not harsh or unpleasantly salty. Add more seasoning only if needed.
- Add the potatoes and cook for 8 to 12 minutes, then add the sausage and cook for 5 minutes.
- Reduce the heat slightly if the pot is violently boiling. Add corn and crab legs; cook for 4 to 7 minutes, just until the corn is tender and the crab is heated through.
- Add lobster tails, mussels, or clams if using. Cook for 4 to 6 minutes, until lobster is opaque and mussels or clams have opened.
- Add shrimp last. Cook for 3 to 5 minutes, just until pink, opaque, and curled into a loose C-shape. For smaller shrimp, turn off the heat and let the covered pot finish them gently.
- Reserve 1 cup / 240 ml seasoned broth, then drain the boil carefully.
- Make the sauce. Melt butter, cook garlic briefly, then stir in Cajun seasoning, paprika, lemon juice, reserved broth, hot sauce if using, and parsley.
- Transfer everything to a large tray or serving platter. Add boiled eggs now if using. Spoon the Cajun garlic butter over the crab joints, corn, potatoes, shrimp, sausage, and eggs, or serve extra on the side for dipping.
Salt note: Cajun seasoning, Old Bay, seafood boil seasoning, and crab boil blends can all contain salt. Start lower if your blend is salty, taste the broth before adding seafood, and adjust slowly.
Success cues:
- Potatoes: tender, but not splitting apart.
- Corn: bright, juicy, and tender when pierced.
- Crab: steaming hot and fragrant.
- Lobster: opaque and firm, not tight.
- Mussels/clams: opened after cooking; discard closed ones.
- Shrimp: pink and curled into a loose C-shape.
- Sauce: shiny, spoonable, and coating instead of watery.

What this recipe is built to prevent: bland potatoes, overcooked shrimp, cold crab, salty broth, watery sauce, and a crowded pot. The timing is staged so the sturdy ingredients get flavor first and the delicate seafood stays tender.

Do not aim for a perfect-looking tray. Aim for hot crab, tender shrimp, juicy corn, potatoes that taste seasoned inside, and enough finishing butter that people start passing bowls around.
Why This Seafood Boil Works
- The broth builds flavor first. Garlic, lemon, onion, bay leaves, and Cajun seasoning get time to season the water before the potatoes go in.
- The pot moves in waves. Potatoes and sausage can handle time; shrimp cannot, so the delicate seafood waits.
- The heat stays steady. A strong boil builds the broth and cooks the potatoes, but seafood does better with a lively simmer or controlled boil.
- The sauce finishes the feast. Reserved broth ties the garlic butter back to the pot, so it tastes like the boil instead of a separate topping.
Make this when you need a messy weekend seafood dinner, a casual birthday tray, a game-day spread, or a restaurant-style boil at home without a giant pot. This is a hands-on dinner, not a quiet plated one: shells cracking, corn turning glossy, potatoes disappearing first, and sauce bowls being passed around the table.
Choose Your Seafood Boil Version
Before you shop, decide what kind of tray you are making. The method stays the same, but this helps you choose the right seafood, sauce level, and pot plan.
| Version | Best for | How to adjust |
|---|---|---|
| Classic shrimp and crab | The all-purpose family-style tray | Use the recipe as written |
| Shrimp-only | Fastest, easiest, most budget-friendly version | Skip crab and use 2.5 to 3 lb / 1.1 to 1.4 kg shrimp |
| Crab-heavy | A special-occasion platter | Use more crab legs and slightly less shrimp |
| Extra saucy | Restaurant-style garlic butter lovers | Use the larger butter sauce option |
| No giant pot | Apartment kitchens or smaller stockpots | Make a half batch or cook in rounds |
Quick Decision Guide
| If this is your situation | Do this |
|---|---|
| First seafood boil | Shrimp + precooked crab, normal sauce, no long soak |
| Small kitchen | Half batch or cook in rounds |
| Mixed spice crowd | Medium broth, hotter sauce on the side |
| Budget version | Shrimp-only with sausage, corn, and potatoes |
| Special occasion | Crab-heavy or add lobster tails |
| Nervous about shrimp | Add shrimp off heat and cover |
Once you choose the version, the rest becomes easier: buy the right seafood, give the pot enough room, and let the sauce make the whole platter feel generous.

Before you shop: for the easiest version, buy raw jumbo shrimp, precooked snow crab legs, smoked sausage, baby potatoes, corn, lemons, garlic, unsalted butter, and one Cajun seasoning you like. Avoid precooked shrimp for the main boil when possible; when that is all you have, add it off heat at the very end just to warm through. Large crab clusters may need a little less total seafood or a two-pot plan.
More help below: ingredients, pot size, seafood per person, seasoning guide, cook order, setup checklist, sauce, no-giant-pot options, storage, troubleshooting, and FAQs.
How This Home Seafood Boil Works
This version is built for a normal home kitchen, not a huge outdoor crawfish pot. Shrimp and crab legs are the default because they are easy to find, quick to cook, and generous on the tray. Crawfish, lobster, mussels, clams, and eggs are optional add-ins, not requirements.
The promise is a bold, saucy seafood platter without special equipment. You season the broth, cook in stages, keep the seafood gentle, and finish everything with Cajun butter.
Ingredients You Need
Ingredients break naturally into four groups: seafood, vegetables, sausage, and sauce. For the lowest-stress first boil, buy raw shell-on shrimp and precooked crab legs. That combination gives you the seafood boil feeling without making the timing complicated.

Shrimp or Prawns
Jumbo shrimp or large prawns work best. Easy-peel or deveined shell-on shrimp are ideal because they hold their texture better, bring more flavor to the broth, and are easier to eat at the table. Peeled shrimp work too, but they cook faster, so add them right at the end.
The best cue is color and shape. Shrimp should be pink, opaque, and curled into a loose C-shape. A tight curl and bouncy texture usually mean they have gone too far. Since shrimp keeps cooking from carryover heat while you drain, sauce, and serve, it waits until the end.
If your shrimp are still frozen and you need a separate no-thaw method for another night, this frozen shrimp in air fryer guide is useful for timing, size cues, and checking whether the shrimp is raw or already cooked.

Crab Legs or Crab Clusters
Snow crab legs are the easiest way to make the tray feel generous without making the cooking harder. They are sweet, easy to crack open at the table, and usually sold already cooked, which means you are mostly warming them through.
King crab legs work too, but they are larger, pricier, and need more room in the pot. Very large clusters are easier to manage in a 12-quart pot or in two rounds.
Still-icy crab legs need a head start. Add them before the corn or give them a few extra minutes before the shrimp goes in, so you do not end up choosing between cold crab and overcooked shrimp.
Raw crab needs proper cooking time. Precooked crab needs gentle reheating so the meat stays sweet instead of dry.
Crawfish, Lobster, Mussels, or Clams
Crawfish is classic in many Louisiana-style boils, but this recipe is written mainly around shrimp and crab. Add crawfish, lobster tails, mussels, or clams only when you know whether they are fresh, frozen, raw, or precooked.
For mussels and clams, discard any that stay open after a firm tap before cooking, and discard any that stay closed after cooking.
Smoked Sausage or Andouille
Andouille gives the most classic smoky Cajun-style flavor, but any good smoked sausage can work. Cut it into thick rounds so it stays juicy. As it simmers, the sausage releases smoky flavor into the broth, and the potatoes and corn pick that up.
Corn and Potatoes
Baby potatoes are ideal because they hold their shape and soak up the Cajun broth. If your potatoes are larger, cut them in half. They are ready when a knife slides in with light resistance, not when they are breaking apart.
Corn adds sweetness and gives you those buttery, spicy bites that make the tray feel complete. The potatoes are often the sleeper hit; give them enough time in the broth and they taste seasoned all the way through.
Onion, Garlic, Lemon, and Bay Leaves
These aromatics turn seasoned water into a proper boil broth. Garlic gives depth, lemon brightens the seafood, onion adds sweetness, and bay leaves bring a gentle savory background note.
When the steam smells like lemon, garlic, bay, and pepper, the pot is ready for the potatoes.
What Size Pot Do You Need for a Cajun Seafood Boil?
A 10 to 12 quart / 9.5 to 11.4 L stockpot is the best home-kitchen size for this recipe. You need enough space for liquid, potatoes, corn, sausage, crab legs, shrimp, and bubbling room.
Keep the pot no more than about two-thirds full once everything is inside. A crowded pot makes the cook nervous; a roomy pot makes the tray better.
| Batch size | Suggested pot size | Best for |
|---|---|---|
| 2 to 3 people | 6 to 7 qt / 5.7 to 6.6 L | Shrimp, sausage, corn, potatoes |
| 4 to 6 people | 10 to 12 qt / 9.5 to 11.4 L | Shrimp and crab legs |
| 6 to 8 people | 16 qt / about 15 L | A fuller boil with extra shellfish |
| 8+ people | 20 to 30 qt / 19 to 28 L | Party-size seafood boil or crawfish boil |
A smaller pot does not mean a smaller dinner. Cook in smarter rounds and let the finishing sauce make everything feel like one big tray. You do not need outdoor equipment for this version. The tray is what makes it feel abundant, not the size of the pot.


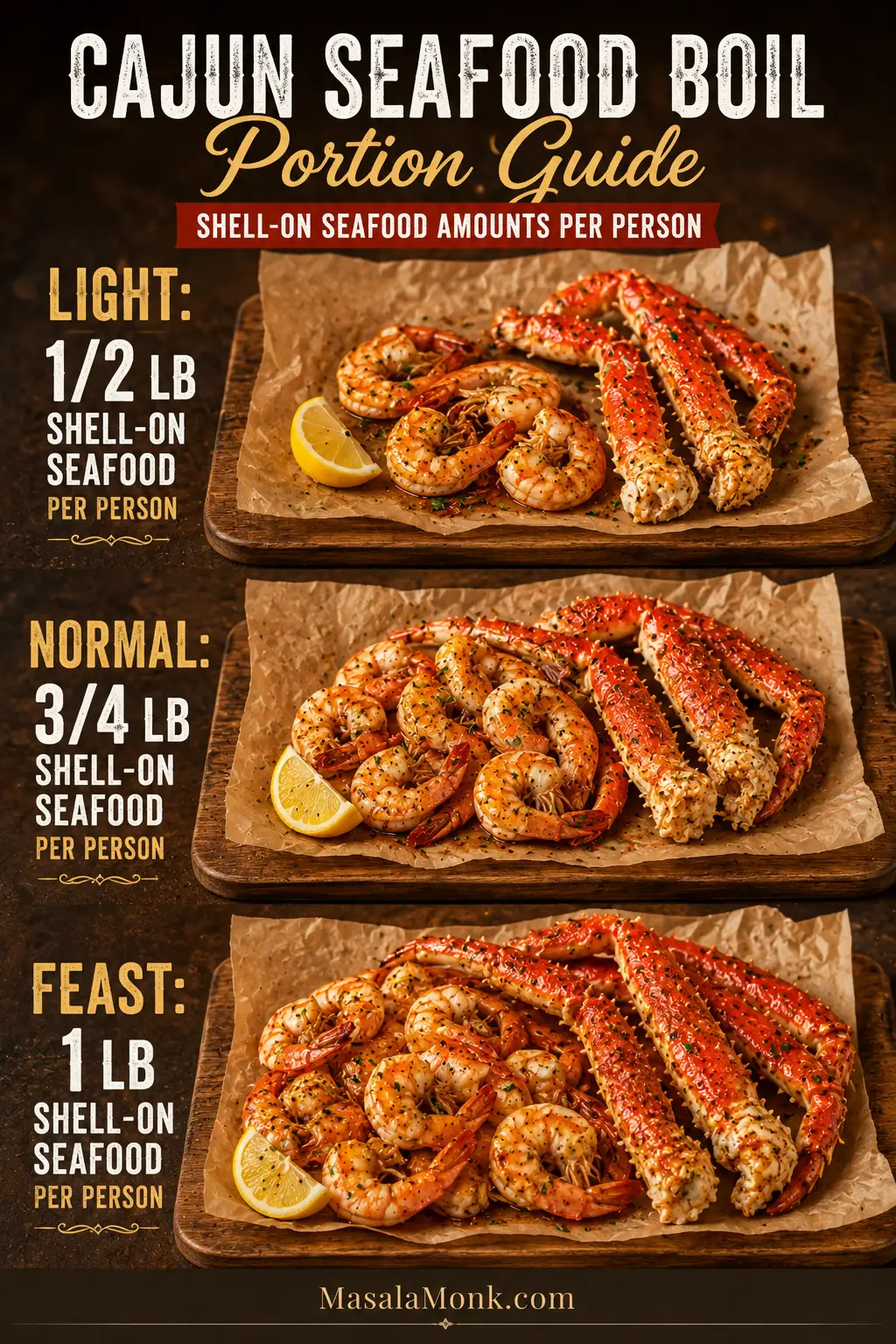
How Much Seafood Per Person?
Shell-on seafood looks generous on the tray, but the shells also count toward the weight. A pound of crab legs or shell-on shrimp does not mean a pound of edible meat.
| Appetite | Seafood per person | Good for |
|---|---|---|
| Light meal | 1/2 lb / 225 g shell-on seafood | Smaller servings with plenty of sides |
| Normal seafood boil | 3/4 lb / 340 g shell-on seafood | Most home boils |
| Big feast | 1 lb / 450 g shell-on seafood | Hungry guests or seafood-heavy meals |
A good 6-person mix is about 2 lb / 900 g crab legs plus 1.5 to 2 lb / 680 to 900 g shrimp. Add crawfish, lobster, mussels, or clams by reducing the shrimp or crab slightly, not by overfilling the pot.
Cajun Seasoning vs Seafood Boil Seasoning vs Old Bay
Seasoning can turn too salty here. Cajun seasoning, seafood boil seasoning, Old Bay, crab boil packets, and liquid crab boil are not always interchangeable in equal amounts.
| Seasoning | What it usually tastes like | How to use it here |
|---|---|---|
| Cajun seasoning | Paprika, garlic, onion, pepper, herbs, cayenne; salt level varies | Main seasoning base |
| Seafood boil seasoning | Often stronger and saltier; made for large pots of water | Use carefully and taste the broth |
| Old Bay | Celery salt-forward seafood seasoning with warm spices | Good as a supporting seasoning |
| Creole seasoning | Similar to Cajun seasoning, often herbier and sometimes milder | Can replace Cajun seasoning if needed |
| Liquid crab boil | Very concentrated, spicy, and aromatic | Use only a small amount if you know the product |
Seasoning the water should smell exciting; it should not make you wince. Choose one main seasoning base, then build slowly. A salt-free Cajun blend may need more salt. A salted Cajun blend plus Old Bay or seafood boil seasoning may not need any extra salt.

Before adding the seafood: taste a spoonful of the broth. It should taste stronger than soup because it has to season potatoes, corn, shells, and seafood, but it should not taste harsh or unpleasantly salty.
Quick Homemade Cajun Seafood Boil Seasoning
For a quick salt-aware blend, keep the seasoning unsalted at first when using Old Bay, seafood boil seasoning, or salted stock.
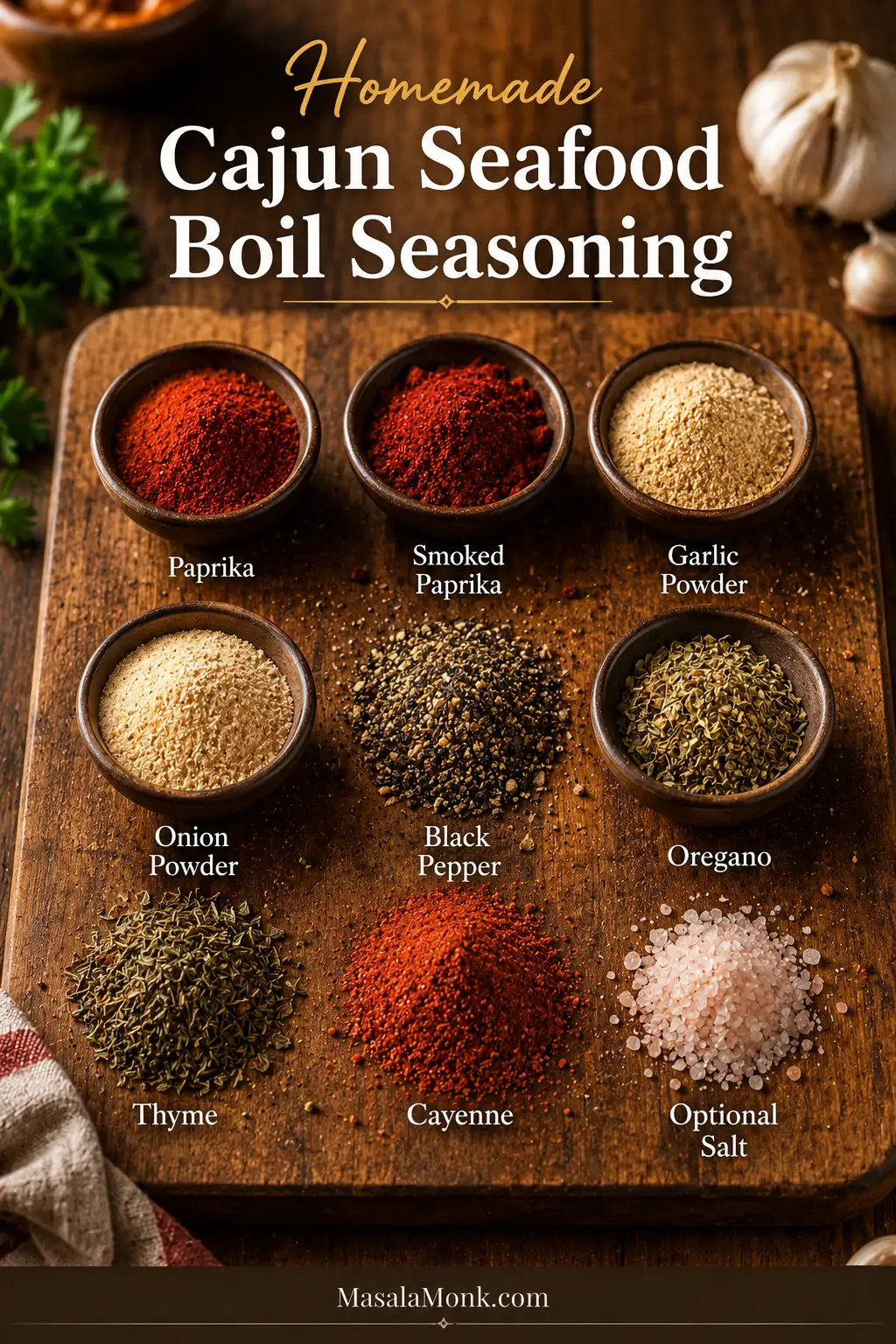
- 2 tablespoons paprika
- 1 tablespoon smoked paprika
- 1 tablespoon garlic powder
- 1 tablespoon onion powder
- 2 teaspoons black pepper
- 1 teaspoon dried oregano
- 1 teaspoon dried thyme
- 1/2 to 2 teaspoons cayenne pepper, to taste
- Optional salt, only if you are not using salty seasoning elsewhere
This homemade blend works well as the Cajun seasoning base. Start with 1/4 cup in the boil broth, taste, then add more if needed. For the butter sauce, use 1 tablespoon of the blend, then adjust heat with hot sauce or cayenne.
Big Seafood Boil Mistakes to Avoid
Most seafood boil problems start before the tray ever reaches the table. Keep these habits in mind and the whole recipe becomes easier.
- Add in stages, not all at once. Potatoes need time, but shrimp does not.
- Build seasoning slowly. Cajun seasoning, Old Bay, crab boil, and seafood boil blends can all bring salt.
- Give the pot room. Crowding drops the temperature, slows cooking, and makes stirring difficult.
- Steady the boil. Use a strong boil for the broth and potatoes, then a gentler boil once seafood goes in.
- Keep shrimp gentle. Add it last and stop when it is no longer translucent and has curled loosely.
- Save some broth. A little seasoned broth makes the butter taste connected to the boil.
- Reheat gently later. Reboiling cooked seafood usually makes it tough.
Think of the pot in waves. The sturdy things go first, the delicate things wait, and the spicy butter brings everyone together at the end.
Cajun Seafood Boil Cook Order Chart
This is the part that saves the seafood. The pot should feel organized, not rushed: potatoes first, shrimp last, and everything else in between.

Use the chart, then trust the cues. The minutes help you plan, but the best seafood boil is still cooked by watching the pot.
| Step | Add | Time | What to watch for |
|---|---|---|---|
| 1 | Water or water-beer mix, onion, garlic, lemon, bay leaves, seasoning | Boil 5 to 10 min | Broth smells bold, garlicky, lemony, and fragrant |
| 2 | Baby potatoes | 8 to 12 min | Knife slides in with light resistance |
| 3 | Sausage | 5 min | Smoky aroma begins seasoning the broth |
| 4 | Corn and precooked crab legs | 4 to 7 min | Corn bright and juicy; crab steaming hot |
| 5 | Lobster tails, mussels, or clams, if using | 4 to 6 min | Lobster opaque; mussels/clams opened |
| 6 | Shrimp or prawns | 3 to 5 min | Pink, opaque, and curled into a loose C-shape |
| 7 | Drain, reserve broth, toss with sauce | 5 min | Everything glossy, hot, and coated |
Small or peeled shrimp are easier to overcook. Turn off the heat before adding them, cover the pot, and let them cook gently in the residual heat for more control.
Should You Soak Seafood Boil Before Draining?
A short soak can help seafood, potatoes, corn, and sausage absorb more flavor from the broth. The risk is shrimp sitting too long in very hot liquid.
For this home version, the safest default is to cook the shrimp until just done, reserve broth, drain, and finish with garlic butter sauce.
For deeper boil flavor, use a controlled short soak. Turn off the heat once the shrimp is nearly done and let the bubbling settle for a minute. If the broth is still very hot and active, add a handful of ice or a splash of cold water, cover the pot, and let everything sit for 5 to 10 minutes. Then reserve broth, drain, and sauce.
Best soak rule: short soak for shrimp-heavy boils, longer soak only if the pot is mostly crab, crawfish, potatoes, corn, and sausage. Avoid hot-soaking small peeled shrimp for a long time.
Set Up Before You Drain
Seafood boils move fast at the end. Set the table before you drain the pot so the tray can go out hot, glossy, and ready to eat.

| You need | Why it helps |
|---|---|
| Large tray, sheet pan, or paper-lined table | Gives the boil room to spread out |
| Spider strainer or tongs | Helps lift seafood without breaking it |
| Crab crackers or kitchen shears | Makes crab easier to eat |
| Shell bowl | Keeps the table usable |
| Napkins or wet towels | Seafood boils are messy |
| Extra lemon and warm butter | Lets people finish their own bites |
How to Make Cajun Seafood Boil
1. Prep Everything Before You Start
Once the pot is hot, things move quickly. Cut the corn into halves or thirds, slice the sausage, halve the lemons, cut the garlic heads across the middle, rinse the seafood, and thaw frozen seafood if needed.
Check your seafood before it goes near the pot. Precooked crab legs need gentle heating. Raw lobster needs enough time to turn opaque. Peeled shrimp cook faster than shell-on shrimp. Mussels and clams should be cleaned and checked carefully.
Seafood is simple to cook, but it is still worth handling carefully. For general buying, thawing, and handling guidance, the FDA has a helpful guide to selecting and serving fresh and frozen seafood safely.
2. Build the Cajun Boil Broth
Add the water or water-beer mix, onion, garlic, lemons, bay leaves, Cajun seasoning, and optional Old Bay to your stockpot. Bring it to a rolling boil, then let it boil for 5 to 10 minutes before adding the main ingredients.

This short simmer wakes up the garlic, lemon, onion, bay leaves, and spices. The broth should smell garlicky, lemony, and spicy before the potatoes go in.
3. Add the Potatoes First
Add the baby potatoes and cook for 8 to 12 minutes. They should be starting to soften but not falling apart. Larger potatoes should be halved so they cook more evenly.

Give this step its time. A knife should slide in with light resistance. When the potatoes get enough time in the broth, they become the bites people keep stealing from the tray.
4. Add the Sausage
Add the sliced sausage and cook for about 5 minutes. The broth should start smelling smoky and savory. Taste again here and adjust carefully if needed.

5. Add the Corn and Crab Legs
Add the corn and crab legs. Cook for 4 to 7 minutes, depending on size. Most frozen crab legs are already cooked, so you are heating them through rather than cooking them aggressively.

Large crab clusters may need a little extra time. Smaller clusters should stay on the shorter side so they remain sweet and tender. If the pot looks angry instead of lively, lower the heat slightly before the delicate seafood goes in.
6. Add Optional Lobster, Mussels, or Clams
Lobster tails, mussels, and clams should go in after the crab has started heating. Lobster tails usually need about 4 to 6 minutes, depending on size. Mussels and clams are done when they open.
Discard any mussels or clams that do not open after cooking. Do not force them open and eat them.
7. Add the Shrimp Last
Shrimp should be the final ingredient. Add it to the hot broth and cook for 3 to 5 minutes, just until pink, opaque, and gently curled. Large shell-on shrimp can handle a few minutes of simmering. Smaller peeled shrimp should be cooked more gently.

For extra control, turn off the heat, add the shrimp, cover the pot, and let the residual heat cook them. This is especially helpful for small shrimp or nervous first-time boils.
8. Reserve Broth, Drain, and Sauce
Scoop out 1 cup / 240 ml of the seasoned broth before draining. Use some of it in the garlic butter sauce. Drain the boil carefully, then transfer everything to a large tray, sheet pan, or paper-lined table.

Pour the Cajun butter over the tray and toss gently, or serve the dip on the side. Spoon extra over the crab joints, corn, potatoes, shrimp, sausage, and boiled eggs if using.
Cajun Garlic Butter Sauce
The broth gives the boil its backbone, but the butter sauce is what people remember. It catches in the crab shells, glosses the shrimp, and turns the potatoes and corn into the bites people keep reaching for.
The sauce is not just decoration here. It is the final seasoning layer, the dip, and the thing that makes the potatoes and corn disappear first.

A good sauce should run off a spoon in a smooth stream and leave a buttery coating behind.
If it looks thin and watery, simmer briefly or add more butter. If it feels heavy or salty, loosen it with unsalted broth or water and brighten it with lemon.

For a coated tray, use the normal sauce. For sauce bowls and extra dipping, double it.
Normal Coating Sauce
This amount is enough to coat a 6-serving seafood tray without drowning it.
| Ingredient | Amount |
|---|---|
| Unsalted butter | 1 cup / 227 g |
| Garlic | 6 to 8 cloves, minced |
| Cajun seasoning | 1 tablespoon |
| Smoked paprika | 1 teaspoon |
| Lemon juice | 1 to 2 tablespoons |
| Reserved boil broth | 1/4 to 1/2 cup / 60 to 120 ml |
| Hot sauce | Optional, to taste |
| Parsley | 2 tablespoons, chopped |
Extra Saucy Restaurant-Style Version
Use this version for a very buttery platter with plenty of dipping sauce.
| Ingredient | Amount |
|---|---|
| Unsalted butter | 2 cups / 454 g |
| Garlic | 8 to 10 cloves, minced |
| Cajun seasoning | 2 tablespoons |
| Old Bay or seafood seasoning | 1 tablespoon, optional |
| Reserved boil broth | 1/2 to 1 cup / 120 to 240 ml |
| Lemon juice | 2 tablespoons |
| Hot sauce | Optional, to taste |
| Brown sugar | Optional pinch, for balance |
| Parsley | 1/4 cup, chopped |
How to Make the Sauce
Melt the butter in a saucepan over medium-low heat. Add the garlic and cook for 30 to 60 seconds, just until fragrant. Keep the garlic pale; deeply browned garlic can make the sauce bitter.

Stir in Cajun seasoning, smoked paprika, lemon juice, and a little reserved broth. Add hot sauce for more heat. Simmer gently for 1 to 2 minutes, then stir in parsley. The sauce should coat the spoon before it coats the tray.
Taste the reserved broth before adding it to the sauce. If the broth is very salty, use water or unsalted stock instead. A flat sauce needs lemon; an intense sauce needs more butter or broth.
Coating Sauce vs Dipping Sauce
A coating sauce uses less broth so the butter clings to the seafood, corn, and potatoes. For a dipping sauce, add a little more broth so it stays loose and spoonable. You can also split it: toss half with the boil and serve the rest in small bowls at the table.
For the saucy restaurant-style finish, do not pour all the butter in one spot. Pour slowly, toss gently, and let it run into the crab joints, between the corn pieces, across the potatoes, and around the shrimp.

If garlic butter shrimp is the part of the tray you love most, this shrimp scampi recipe gives you the same lemon-garlic-butter comfort in a quicker pasta-friendly format.
Make-Ahead and Leftover Sauce
You can make the butter sauce 2 to 3 days ahead. Store it in the refrigerator, then rewarm it gently over low heat. Add a splash of reserved broth, stock, or water if it thickens too much.
Leftover sauce is worth saving. Spoon it over shrimp, crab legs, lobster tails, corn, potatoes, garlic bread, roasted vegetables, rice, or pasta. Freeze extra sauce in small portions for an easy Cajun butter finish another day.
That extra bowl is also excellent with torn pieces of homemade garlic bread, especially when you need something simple to catch the spicy, lemony butter.
No Giant Pot? Here Are Your Options
The classic version can be huge, but a normal kitchen can still make a satisfying batch. The tray does not care whether everything cooked in one pot. The sauce makes it feel united.
Option 1: Split the Recipe Between Two Pots
If you have two medium stockpots, divide the broth, potatoes, corn, sausage, and seafood between them. Keep the timing the same, but watch each pot separately. This is the easiest way to make the full recipe without overcrowding one pot.
Option 2: Make a Half Batch
For 2 to 3 people, cut the recipe in half and use a 6 to 7 quart / 5.7 to 6.6 L Dutch oven or stockpot. A shrimp-and-crab version works especially well for a smaller batch.
For a quieter seafood dinner with no big pot at all, this baked haddock recipe follows the same gentle-cooking idea: season well, avoid overcooking, and let the fish stay tender.
Option 3: Boil First, Sauce Later
If your pot is too small for everything at once, cook the potatoes and corn first, remove them, then cook the seafood separately. Combine everything on a tray and pour the hot Cajun garlic butter sauce over the top. You still get the same messy, saucy feeling without needing a massive pot.

What About a Seafood Boil Bag?
For a seafood boil bag, use this same seasoning and sauce logic, but treat it as a separate oven-bag method: cooked potatoes and corn, raw shrimp added late, and sauce sealed in or tossed after cooking. This stovetop version gives more classic broth flavor because everything cooks in seasoned liquid.
Seafood Swaps and Variations
Use the seafood that is fresh, available, and reasonably priced where you live. The pot does not need to look exactly like anyone else’s; it just needs to be timed well and sauced generously.
| If you do not have | Use this instead |
|---|---|
| Crawfish | Shrimp, prawns, crab legs, or lobster tails |
| Snow crab | King crab, blue crab, local crab, or extra shrimp |
| Andouille | Smoked sausage, chicken sausage, or chorizo-style sausage |
| Old Bay | A little extra Cajun seasoning, celery salt, paprika, garlic powder, and black pepper |
| Mussels or clams | Skip them or add more shrimp and crab |
| Lemon | Lime in a pinch |
| Beer | More water, seafood stock, chicken stock, or vegetable stock |
| Boiled eggs | Skip them or add peeled hard-boiled eggs after draining |
Shrimp-Only Cajun Seafood Boil
For an easier version, skip the crab and use 2.5 to 3 lb / 1.1 to 1.4 kg large shell-on shrimp. Keep the potatoes, corn, sausage, and garlic butter sauce. Add the shrimp at the very end so it does not overcook.
For another quick shrimp dinner where timing matters just as much, these shrimp tacos use the same idea: cook the shrimp hot and fast, then build the fresh parts around it.
Crab-Lovers Seafood Boil
Use 3 to 4 lb / 1.4 to 1.8 kg crab legs and reduce the shrimp slightly. Since crab legs are usually precooked, focus on heating them gently and coating them well with Cajun butter.
Crawfish-Style Boil
If crawfish is available, add it with or shortly before the shrimp, depending on whether it is fresh, frozen, raw, or precooked. Crawfish boils often use stronger seafood boil seasoning, so be extra careful with salt and spice levels.
If crawfish is already cooked, treat it more like crab and warm it gently. If it is raw or live, use crawfish-specific cleaning and cooking guidance rather than relying on the shrimp timing in this recipe. This recipe can borrow crawfish-boil flavors, but it is not a full live-crawfish boil tutorial.
Lobster Tail Upgrade
Add 2 to 3 lobster tails for a more special-occasion boil. Cut the shells slightly so the seasoning and butter can reach the meat. Lobster tails usually need only a few minutes and should be opaque, not tough.
If you end up with extra cooked lobster meat, save it for a buttery lobster roll instead of reheating it hard in the pot again.
Boiled Egg Add-In
Boiled eggs are optional, but they are great on a restaurant-style seafood tray. Add peeled hard-boiled eggs after draining and spoon Cajun butter over them. They do not need to boil with the seafood; they just need the sauce.
How Spicy Should Cajun Seafood Boil Be?
The boil should be bold, but it does not have to be painfully hot. Keep the broth flavorful and serve extra heat in the butter sauce or hot sauce on the side.
- Mild: use less cayenne, skip hot sauce, and rely on paprika, garlic, lemon, and herbs.
- Medium: use regular Cajun seasoning and a small amount of hot sauce in the butter.
- Spicy: add cayenne, hot sauce, or crushed red pepper to the sauce.
- Extra spicy: add more cayenne or a very small amount of liquid crab boil if you know its strength.
- Family-style: keep the pot medium and serve spicy garlic butter separately.
For a mixed group, keep the pot medium and let people add heat at the table. It is easier to make one bowl of sauce hotter than to rescue potatoes, corn, and shrimp that are too spicy for some people to enjoy.
What to Serve With Cajun Seafood Boil
The tray already has protein, potatoes, corn, and sauce, so sides can stay simple. Think fresh, crisp, buttery, or bread-based sides that balance the spice and soak up the sauce.
A cold, crunchy side helps balance the butter and spice. This coleslaw recipe is the cleanest fit when you need something creamy, tangy, and crisp beside the seafood tray.
- Garlic bread or crusty bread for soaking up sauce
- Coleslaw or a crisp cabbage salad
- Green salad with lemony dressing
- Extra lemon wedges
- Pickles or quick-pickled onions
- Steamed rice, if you need to stretch the meal
- Cold drinks, iced tea, lemonade, or beer
To make the meal feel heartier and more Louisiana-style, red beans and rice makes more sense than adding another heavy seafood dish beside it.
For serving, spread the drained boil on a large tray, sheet pan, or paper-lined table. Spoon the garlic butter sauce over everything while it is hot. Keep extra sauce in bowls for dipping crab, shrimp, corn, and potatoes.


Bring the tray to the table while it is hot, saucy, and just cooked. The first crack of crab, the lemon squeezed over the shrimp, and the butter running into the corn are the whole point.
The best part is that everyone has to slow down a little: crack crab, peel shrimp, pass lemon, steal another potato, and reach for the sauce again.
Storage and Reheating
This meal is best served fresh, but leftovers can still be good if you reheat them gently. The main rule is simple: do not reboil cooked seafood. Reboiling usually makes shrimp tough and crab dry.
How to Store Leftovers
- Let leftovers cool, then transfer them to airtight containers.
- Refrigerate for up to 2 days.
- Store extra garlic butter sauce separately if possible.
- Remove seafood from shells before storing if you want easier reheating.
- Do not leave cooked seafood sitting out for long.
Leftovers are where texture and safety both matter. For general leftover safety, the USDA’s leftovers and food safety guide is a useful reference. For this seafood boil, the shorter 2-day window is best for quality and texture.
Best Way to Reheat Seafood Boil
For the best texture, reheat leftovers in a covered skillet over low heat with a spoonful of butter, broth, or sauce. Warm just until heated through. A covered oven-safe dish at low heat also works for larger portions.
The microwave works in a pinch, but use short bursts and low or medium power if possible. Shrimp can go from warm to rubbery quickly.
If you shell extra shrimp before storing, turn it into shrimp fried rice the next day instead of reheating the whole tray again.
Can You Freeze Seafood Boil?
You can freeze cooked seafood, but the texture may change, especially for shrimp and potatoes. Extra sauce freezes better than the full boil, so save that separately when possible.
Troubleshooting Cajun Seafood Boil
If something feels off, do not panic. Most seafood boil problems come down to timing, salt, or heat, and all three are easier to fix when you catch them early.
Why Is My Shrimp Rubbery?
The shrimp was probably added too early, boiled too hard, or cooked too long. Add shrimp last and stop when it is pink, opaque, and gently curled. Smaller shrimp are safer with residual heat than a rolling boil.

Why Are My Potatoes Bland?
The broth may not have been seasoned enough before the potatoes went in, or the potatoes did not spend enough time in the seasoned liquid. Potatoes need a head start so they can absorb flavor from the Cajun broth.
Why Is My Seafood Boil Too Salty?
Salt usually builds up when salted Cajun seasoning, Old Bay, seafood boil seasoning, and extra salt are all used together. Stop adding seasoning.
If the seafood is already cooked, lift it out before fixing the broth. Dilute with unsalted water or stock, taste again, and use unsalted butter and lemon in the sauce to soften the salt.
Why Is My Garlic Butter Sauce Watery?
Too much reserved broth was added. Simmer the sauce gently for a minute or add more butter to bring back richness. For a thicker coating, use less broth and spoon it over the seafood while hot.

Why Did My Garlic Butter Sauce Break?
The heat was probably too high, or too much broth was added too quickly. Keep the butter over medium-low heat and stir in broth gradually. Even if the sauce separates slightly, it will still taste good spooned over the seafood.
Can I Use Frozen Seafood?
Yes. Thaw shrimp and lobster tails before cooking when possible so they cook evenly. Precooked frozen crab legs usually only need to be heated through. Frozen seafood added straight to the pot will drop the broth temperature and may change the timing.
Can I Make Seafood Boil Ahead?
You can prep the vegetables, cut the sausage, clean the seafood, and make the butter sauce ahead. For the best texture, cook the seafood close to serving time. The tray is much better freshly cooked than reheated for a crowd.
FAQs About Cajun Seafood Boil
What seafood is best for a Cajun seafood boil?
Shrimp and crab legs are the easiest home combination. Crawfish, lobster tails, mussels, and clams also work if you know whether they are raw, frozen, fresh, or precooked.
What seasoning do you use for Cajun seafood boil?
Use Cajun seasoning as the main flavor base. A little Old Bay or seafood boil seasoning can help, but check salt levels first. The broth should taste bold, not sharp or salty.
Is Cajun seasoning the same as seafood boil seasoning?
Not exactly. Cajun seasoning is usually a spice blend with paprika, garlic, onion, herbs, pepper, and cayenne. Seafood boil seasoning is often stronger and saltier because it seasons a large pot of water.
How much Cajun seasoning should I use?
For this 6-serving recipe, start with 1/4 cup. Use up to 1/2 cup only if your blend is low-salt or salt-free. Taste the broth before adding seafood.
Should I use salted or unsalted butter?
Use unsalted butter if possible. The broth and seasonings already bring salt, so unsalted butter gives you room to adjust the final sauce.
Do I need beer in a seafood boil?
No. Beer adds depth, but water works. Seafood stock, chicken stock, or vegetable stock can make the broth taste fuller.
What order do you add seafood boil ingredients?
Start with seasoned broth, then add potatoes, sausage, corn and crab, optional lobster or shellfish, and shrimp last. Think sturdy to delicate.
How long should shrimp cook in a seafood boil?
Large shrimp usually need 3 to 5 minutes. They are done when pink, opaque, and gently curled. Smaller shrimp can finish off heat in the covered pot.
Do crab legs need to be cooked or just reheated?
Most frozen crab legs sold at grocery stores are already cooked, so they only need reheating. Raw crab needs proper cooking time.
Should I thaw frozen shrimp before seafood boil?
Yes, thaw shrimp when possible. Thawed shrimp cook more evenly and are easier to time. Frozen shrimp drops the broth temperature and may cook unevenly.
Can I use precooked shrimp?
Yes, but raw shrimp is better for the main boil. Add precooked shrimp off heat at the very end and let the covered pot warm it gently.
What sausage works best?
Andouille is classic, but any smoky sausage that holds its shape can work.
How do you make Cajun garlic butter sauce?
Melt unsalted butter over medium-low heat, cook minced garlic briefly, then stir in Cajun seasoning, smoked paprika, lemon juice, a little reserved broth, hot sauce, and parsley.
How do I make seafood boil less spicy?
Use less cayenne, skip hot sauce, and choose a mild Cajun seasoning. Keep the broth medium and serve hotter butter on the side.
What can I use instead of crawfish?
Shrimp and crab legs are the easiest substitute. Lobster tails, mussels, or clams can make the tray feel fuller.
Can I add boiled eggs to seafood boil?
Yes. Add peeled hard-boiled eggs after draining and spoon Cajun garlic butter over them. They do not need to boil with the seafood.
Can I make seafood boil in a bag?
Yes, but treat it as a different method. Use cooked potatoes and corn, add raw shrimp late, and use Cajun butter as the finishing sauce. The stovetop version gives more broth flavor.
How do you keep seafood boil warm for serving?
Keep the drained seafood, potatoes, corn, and sausage on a warm tray loosely covered with foil. Hold extra butter warm separately and spoon it over right before serving.
How do you make seafood boil without a large pot?
Make a half batch, split the recipe between two pots, or cook in rounds and combine everything on a tray with hot Cajun butter.
How do you reheat seafood boil leftovers?
Reheat gently in a covered skillet with a little butter, broth, or sauce. Warm just until hot so the seafood does not cook a second time.
Final Tips for the Best Cajun Seafood Boil
The secret to a good Cajun seafood boil is calm control: bold broth, patient potatoes, gentle seafood, and butter sauce at the end. Keep extra lemon nearby, adapt the seafood based on what is available, and avoid overcrowding the pot just to make the tray look bigger.
Do not worry about making it look perfect. A seafood boil is supposed to look abundant, saucy, and a little chaotic. That is part of the fun.
When everything comes together, you get the kind of meal people lean into: crab shells cracking, shrimp dipped in spicy butter, corn dripping with sauce, potatoes soaked with Cajun broth, and a table that feels full before anyone even takes the first bite.
If you make it, tell me what went into your tray and what you changed: shrimp and crab, lobster tails, extra sausage, more spice, less spice, no giant pot, boiled eggs, or the full feast. Those details help the next reader plan their own boil.